
Thank you for joining us for another look at how to get the most out of reporting in UKG Clinical Scheduling Extensions (formerly Kronos Workforce Scheduler Extensions for Healthcare). My goal is for this content to help you make more effective decisions both in real time and for future needs!
In my last post, I showed you how to view and analyze patient and staff workload at the unit level and up through your entire organization. Today, we will tackle something on the minds of many within your organization — budget and productivity metrics!
So, things are going well with your system. Staff love how it gives them credit for all the care they provide. Clinical leadership at the unit and departmental levels up to the CNO love having real-time and historical documentation that patients receive the care they need when they need it and that resources are utilized in the most efficient way possible. Wonderful! But are you staying within budget? Can you see when and where staff is busiest and why? Do you have the tools to identify issues and course-correct before they get out of hand?
Guess what? You do! Let’s have a look.
Tip: If you need to reference a glossary of terms, skip to the end.
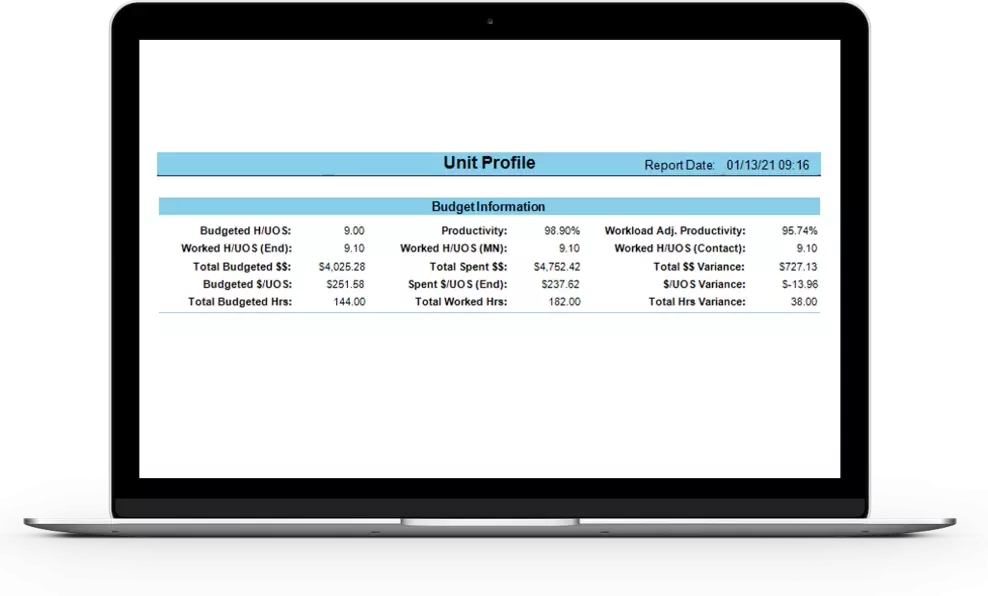
Unit Profile Report
We told you it would be back! You have already learned how this comprehensive report provides valuable information on unit workload as well as a way to assess system utilization and demonstrate compliance with various organizational staffing and care need requirements. Now let’s see how you can leverage it to evaluate unit-specific budget and productivity metrics.
Budget information — The budget information section of the Unit Profile Report shows financial and productivity data for the timeframe selected by comparing static budgeted hours per unit of service (you may know this as hours per patient day) with three different patient census perspectives:
- Midnight
- End
- Contact
What are these? Glad you asked! Let’s start with the midnight census, as it is the most familiar to users. The midnight census is the number of patients in the unit at the end of the 24-hour day. Although this is a valuable metric and is commonly used by the finance department when reviewing a unit’s daily actual versus budgeted spend, it does not always provide a complete picture of the overall unit workload. That is why the Unit Profile Report also looks at worked hours based on the end census and the contact census. The end census is the average census at the end of each shift included in the report. The contact census is the total number of patients seen in the unit during the period reviewed regardless of their length of stay. Where the midnight census provides the “end-of-day” worked Hours per Unit of Service, contact and end census take unit churn or throughput into consideration, capturing the work of all the transfers in and out of the unit.
Productivity percentage — Divide the static budgeted hours per unit of service by the end worked hours per unit of service to calculate productivity percentage. This calculation is a great visual of how busy the unit was during the period reviewed. If the productivity percentage is less than 100%, the worked hours per unit of service was more than what the unit was budgeted for. In other words, staff can spend more time than expected with each of their patients. On the other hand, when the productivity percentage is more than 100%, that means staff have been assigned more patients and cannot spend as much time with each of them. Productivity is up because they are caring for or seeing more patients in the same amount of time.
Workload-adjusted productivity percentage — When the Workload Manager component of your UKG Clinical Scheduling Extensions solution is configured, this report also provides a workload-adjusted productivity percentage. The productivity percentage is based on actual census, while the workload-adjusted productivity percentage value takes into account patient workload and the heaviness of the care they require. So, even though a unit has an actual census of 20 patients, it feels like staff is caring for 24 patients because some of them have a higher-than-expected workload. The workload-adjusted productivity percentage is based on this census value, giving users a more realistic picture of unit workload and needs.
Dollars per unit of service — The Unit Profile Report also details dollars per unit of service (per patient day). By dividing the value for a unit’s budgeted dollars per patient day by the number of days you are running the report, users can get the average spend per patient who received care. The report also includes actual versus budgeted total spend for the reporting period.
Unit Productivity Report
As the name implies, the Unit Productivity Report shows how efficiently resources are utilized by comparing a unit’s budgeted census with the actual number of patients seen. It does the same for budgeted versus actual hours, hours per unit of service, and dollars spent — including a cumulative variance for a selected date range for these metrics so you can see precisely when values begin to skew and course-correct accordingly.
Just like the Unit Profile Report, this report allows you to compare the unit’s static budgeted census with its actual contact, end, or midnight census. You can also run this report with the projected census (the expected number of patients for a given period) or the blended census (an average of the census for each hour the report is run). These last two metrics often help determine needs for units with high turnover or large fluctuations in census levels.

The Unit Productivity Report can be run to show only direct care hours or to include all productive roles in the unit.
Staffing Analysis Report
The Staffing Analysis Report provides much of the data seen in the Unit Productivity Report with the addition of nurse staffing ratios. Budgeted versus actual midnight, projected, end, and contact census values are available as well as the unit’s productivity percentage and a comparison of budgeted hours with actual hours worked. Just like the Unit Profile Report, you can view the productivity percentage based on the actual number of patients in the unit or based on how many patients it feels like you’re caring for in the unit, which captures the overall work required to care for each patient. This helps answer why staff seemed overworked when the actual census was so close to the budgeted one. They may have only had 20 patients, but because of the increased workload, it felt like they were caring for 25.
Indexes section — Users can better understand how busy the unit has been by reviewing the Indexes section of the report. The workload index is the average workload weight of all patients who have been in the unit, even those who were transferred out. A value of 1 means all patients were an average or expected workload for the unit. Anything more than 1 means the unit was busier than expected for the period reviewed. The admissions, discharges, and transfers index takes the total number of transfers in and out of the unit and divides it by the contact census to show unit turnover. Since moving patients adds to unit workload, this metric helps provide a more comprehensive picture of your overall productivity.
Staffing ratios for licensed care providers — Last but not least, the Staffing Analysis Report includes staffing ratios for the unit’s licensed care providers. The report looks at the total number of minutes patients were in the unit and the total amount of time staff was scheduled to work during the shift. It also compares the midnight census with the number of licensed staff per day to give a per-shift daily breakdown of how many patients each nurse cared for. This section also includes metrics that take the workload-adjusted census into account.

Final thoughts
Ensuring patients receive quality care from the right resources at the right time is everyone’s priority. However, unit and organizational leadership must also consider the financial impact of their decisions. Fortunately, UKG Clinical Scheduling Extensions give you the tools to view the impact unit status has on your budget and demonstrate why there are variances and when you need to make adjustments to stay on track.
I hope that this review of reports has been useful and will help ensure you are getting the most out of your solution. Tune in next time, when we will show how you can record staffing needs with reports!
More blogs about reporting for UKG Clinical Scheduling Extensions:
- How to Review Patient and Staff Workload in Workforce Scheduler Extensions
- Getting the Most out of Workforce Scheduler Extensions Reports
- Optimizing Usage of Workforce Scheduler Extensions — Leveraging Reports
Glossary of Key Terms
- Unit profile report: provides valuable information on unit workload as well as a way to assess system utilization and compliance
- Budget information: shows financial and productivity data by comparing budgeted hours per unit of service with midnight census, end census, or contact census
- Midnight census: the number of patients in the unit at the end of the 24-hour day
- End census: the average census at the end of each shift included in the report
- Contact census: the total number of patients seen in the unit during the period reviewed, regardless of their length of stay
- Productivity percentage: calculated by dividing the static budgeted hours per unit of service by the end worked hours per unit of service; demonstrates how busy the unit was during the period reviewed; based on actual census
- Workload-adjusted productivity percentage: productivity percentage that considers patient workload and the heaviness of the care they require; provides a more realistic picture of unit workload and needs
- Dollars per unit of service: divide a unit’s budgeted dollars per patient day by the number of days in the report period; provides average spend for each patient who received care
- Unit productivity report: shows how efficiently resources are utilized by comparing a unit’s budgeted census with the actual number of patients seen
- Staffing analysis report: provides much of the data seen in the Unit Productivity Report with the addition of staffing ratio information
- Workload index: the average workload weight of all patients who have been in the unit, even those who were transferred out
- Admissions, discharges, and transfers index: takes the total number of transfers in and out of the unit and divides it by the contact census to show unit turnover
- Staffing ratios for care providers: provides staffing ratios for the unit’s licensed care providers